Pramipexole hydrochloride.
Ramipex 0.25: Each tablet contains: Pramipexole hydrochloride 250 mcg (equivalent to pramipexole 180 mcg).
Ramipex 1: Each tablet contains: Pramipexole hydrochloride 1 mg (equivalent to Pramipexole 700 mcg).
Pharmacology: Pharmacodynamics: Mechanism of Action: Pramipexole is a non-ergot dopamine agonist with high relative in vitro specificity and full intrinsic activity at the D2 subfamily of dopamine receptors, binding with higher affinity to D3 than to D2 or D4 receptor subtypes.
The precise mechanism of action of pramipexole as a treatment for Parkinson's disease is unknown, although it is believed to be related to its ability to stimulate dopamine receptors in the striatum. This conclusion is supported by electrophysiologic studies in animals that have demonstrated that pramipexole influences striatal neuronal firing rates via activation of dopamine receptors in the striatum and the substantia nigra, the site of neurons that send projections to the striatum. The relevance of D receptor binding in Parkinson's disease is unknown.
Pharmacokinetics: Pramipexole displays linear pharmacokinetics over the clinical dosage range. Its terminal half-life is about 8 hours in young healthy volunteers and about 12 hours in elderly volunteers. Steady-state concentrations are achieved within 2 days of dosing.
Absorption: Pramipexole is rapidly absorbed, reaching peak concentrations in approximately 2 hours. The absolute bioavailability of pramipexole is greater than 90%, indicating that it is well absorbed and undergoes little presystemic metabolism. Food does not affect the extent of pramipexole absorption, although the time of maximum plasma concentration (Tmax) is increased by about 1 hour when the drug is taken with a meal.
Distribution: Pramipexole is extensively distributed, having a volume of distribution of about 500 L (coefficient of variation [CV]=20%). It is about 15% bound to plasma proteins. Pramipexole distributes into red blood cells as indicated by an erythrocyte-to-plasma ratio of approximately 2.
Metabolism: Pramipexole is metabolized only to a negligible extent (<10%). No specific active metabolite has been identified in human plasma or urine.
Elimination: Urinary excretion is the major route of pramipexole elimination, with 90% of a pramipexole dose recovered in urine, almost all as unchanged drug. The renal clearance of pramipexole is approximately 400 mL/min (CV=25%), approximately three times higher than the glomerular filtration rate. Thus, pramipexole is secreted by the renal tubules, probably by the organic cation transport system.
Pharmacokinetics in Specific Populations: Because therapy with pramipexole dihydrochloride tablets are initiated at a low dose and gradually titrated upward according to clinical tolerability to obtain the optimum therapeutic effect, adjustment of the initial dose based on gender, weight, race, or age is not necessary.
However, renal insufficiency, which can cause a large decrease in the ability to eliminate pramipexole, may necessitate dosage adjustment.
Gender: Pramipexole clearance is about 30% lower in women than in men, but this difference can be accounted for by differences in body weight. There is no difference in half-life between males and females.
Age: Pramipexole clearance decreases with age as the half-life and clearance are about 40% longer and 30% lower, respectively, in elderly (aged 65 years or older) compared with young healthy volunteers (aged less than 40 years). This difference is most likely due to the reduction in renal function with age, since pramipexole clearance is correlated with renal function, as measured by creatinine clearance.
Race: No racial differences in metabolism and elimination have been identified.
Parkinson's Disease Patients: A cross-study comparison of data suggests that the clearance of pramipexole may be reduced by about 30% in Parkinson's disease patients compared with healthy elderly volunteers. The reason for this difference appears to be reduced renal function in Parkinson's disease patients, which may be related to their poorer general health. The pharmacokinetics of pramipexole were comparable between early and advanced Parkinson's disease patients.
Hepatic Impairment: The influence of hepatic insufficiency on pramipexole pharmacokinetics has not been evaluated.
Because approximately 90% of the recovered dose is excreted in the urine as unchanged drug, hepatic impairment would not be expected to have a significant effect on pramipexole elimination.
Renal Impairment: Clearance of pramipexole was about 75% lower in patients with severe renal impairment (creatinine clearance approximately 20 mL/min) and about 60% lower in patients with moderate impairment (creatinine clearance approximately 40 mL/min) compared with healthy volunteers.
In patients with varying degrees of renal impairment, pramipexole clearance correlates well with creatinine clearance. Therefore, creatinine clearance can be used as a predictor of the extent of decrease in pramipexole clearance.
Used in the management of Parkinson's disease either alone or as an adjunct to levodopa therapy to reduce "end-of-dose" or "on-off" fluctuations in response.
General Dosing Considerations: Pramipexole tablets are taken orally, with or without food.
If a significant interruption in therapy with pramipexole tablets have occurred, retitration of therapy may be warranted.
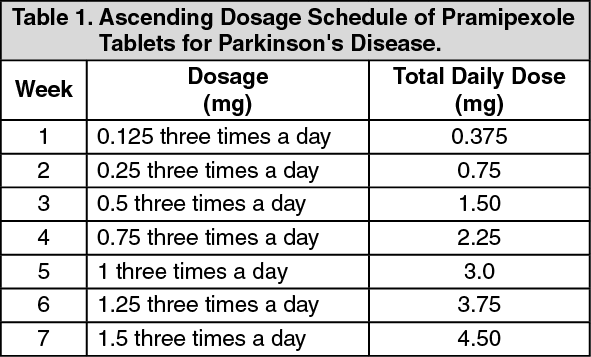
Dosing in Patients with Normal Renal Function: Initial Treatment: Doses should be increased gradually from a starting dose of 0.375 mg/day given in three divided doses and should not be increased more frequently than every 5 to 7 days. A suggested ascending dosage schedule that was used in clinical studies is shown in Table 1 (see Table 1):
 Click on icon to see table/diagram/image
Maintenance Treatment:
Click on icon to see table/diagram/image
Maintenance Treatment: Pramipexole is effective and well tolerated over a dosage range of 1.5 to 4.5 mg/day administered in equally divided doses three times per day with or without concomitant levodopa.
When pramipexole tablets are used in combination with levodopa, a reduction of the levodopa dosage should be considered.
Dosing in Patients with Renal Impairment: The recommended dosing of pramipexole in Parkinson's disease patients with renal impairment is provided in Table 2. (See Table 2.)
Click on icon to see table/diagram/image
Discontinuation of Treatment: Pramipexole may be tapered off at a rate of 0.75 mg per day until the daily dose has been reduced to 0.75 mg. Thereafter, the dose may be reduced by 0.375 mg per day.
Or as prescribed by the physician.
There is no clinical experience with massive overdose. The expected adverse reactions would be those related to the pharmacodynamic profile of a dopamine agonist, including nausea, vomiting, hyperkinesia, hallucinations, agitation and hypotension. There is no established antidote for overdose of a dopamine agonist. If signs of central nervous system stimulation are present, a neuroleptic agent may be indicated. Management of the overdose may require general supportive measures, along with gastric lavage, intravenous fluids, administration of activated charcoal and electrocardiogram monitoring.
Hypersensitivity to Pramipexole or to any of the excipients of the drug product.
Falling Asleep During Activities of Daily Living and Somnolence: Pramipexole has been associated with somnolence and episodes of sudden sleep onset, particularly in patients with Parkinson's disease.
Sudden onset of sleep during daily activities, in some cases without awareness or warning signs, has been reported uncommonly. Patients must be informed of this and advised to exercise caution while driving or operating machines during treatment with Pramipexole. Patients who have experienced somnolence and/or an episode of sudden sleep onset must refrain from driving or operating machines. Furthermore, a reduction of the dose or termination of therapy may be considered. Because of possible additive effects, caution should be advised when patients are taking other sedating medicinal products or alcohol in combination with pramipexole.
Symptomatic Orthostatic Hypotension: Dopamine agonists, in clinical studies and clinical experience, appear to impair the systemic regulation of blood pressure, with resulting orthostatic hypotension, especially during dose escalation.
Parkinson's disease patients, in addition, appear to have an impaired capacity to respond to an orthostatic challenge. For these reasons, Parkinson's disease patients being treated with dopaminergic agonists ordinarily require careful monitoring for signs and symptoms of orthostatic hypotension, especially during dose escalation, and should be informed of this risk. Impulse Control/Compulsive Behaviors Pathological gambling, increased libido and hypersexuality have been reported in patients treated with dopamine agonists for Parkinson's disease, including pramipexole dihydrochloride. Furthermore, patients and caregivers should be aware of the fact that other behavioral symptoms of impulse control disorders and compulsions such as binge eating and compulsive shopping can occur. Dose reduction/tapered discontinuation should be considered.
Hallucinations and Psychotic-like Behavior: Hallucinations are known as a side effect of treatment with dopamine agonists and levodopa. Patients should be informed that (mostly visual) hallucinations can occur.
Patients with a major psychotic disorder should ordinarily not be treated with dopamine agonists, including pramipexole, because of the risk of exacerbating the psychosis. In addition, certain medications used to treat psychosis may exacerbate the symptoms of Parkinson's disease and may decrease the effectiveness of pramipexole.
Dyskinesia: Pramipexole may potentiate the dopaminergic side effects of levodopa and may cause or exacerbate preexisting dyskinesia.
Renal Impairment: Since pramipexole is eliminated through the kidneys, caution should be exercised when prescribing pramipexole to patients with renal impairment.
Ophthalmologic monitoring: Ophthalmologic monitoring is recommended at regular intervals or if vision abnormalities occur.
Neuroleptic malignant syndrome: Symptoms suggestive of neuroleptic malignant syndrome have been reported with abrupt withdrawal of dopaminergic therapy.
Melanoma: Epidemiological studies have shown that patients with Parkinson's disease have a higher risk (2- to approximately 6-fold higher) of developing melanoma than the general population.
Hence, patients and providers are advised to monitor for melanomas frequently and on a regular basis when using pramipexole dihydrochloride tablets for any indication. Ideally, periodic skin examinations should be performed by appropriately qualified individuals (e.g.,dermatologists).
Pregnancy Category C. There are no adequate and well-controlled studies in pregnant women. Pramipexole should be used during pregnancy only if the potential benefit justifies the potential risk the fetus.
It is not known whether this drug is excreted in human milk. Because many drugs are excreted in human milk and because of the potential for serious adverse reactions in nursing infants from pramipexole, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
The effect on pregnancy and lactation has not been investigated in humans. Pramipexole was not teratogenic in rats and rabbits, but was embryotoxic in the rat at maternotoxic doses. Pramipexole (Ramipex) should not be used during pregnancy unless clearly necessary, i.e. if the potential benefit justifies the potential risk to the fetus.
As pramipexole treatment inhibits secretion of prolactin in humans, inhibition of lactation is expected. The excretion of pramipexole into breast milk has not been studied in women. In rats, the concentration of active substance-related radioactivity was higher in breast milk than in plasma.
In the absence of human data, Pramipexole (Ramipex) should not be used during breastfeeding. However, if its use is unavoidable, breast-feeding should be discontinued.
The following adverse reactions are expected under the use of Pramipexole: abnormal dreams, amnesia, behavioral symptoms of impulse control disorders and compulsions such as binge eating, compulsive shopping, hypersexuality and pathological gambling; confusion, constipation, delusion, dizziness, dyskinesia, dyspnea, fatigue, hallucinations, headache, hyperkinesia, hyperphagia, hypotension, insomnia, libido disorders, nausea, paranoia, peripheral edema, pneumonia, pruritus, rash and other hypersensitivity; restlessness, somnolence, sudden onset of sleep, syncope, visual disturbance including vision blurred and visual acuity reduced, vomiting, weight decrease, weight increase.
Within the system organ classes, adverse reactions are listed under headings of frequency (number of patients expected to experience the reaction), using the following categories: very common (≥1/10); common (≥/100 to < 1/10); uncommon (≥1/1,000 to < 1/100); rare (≥1/10,000 to < 1/1,000); very rare (< 1/10,000); not known (cannot be estimated from the available data).
Parkinson's disease, most common adverse reactions: The most commonly (≥5%) reported adverse drug reactions in patients with Parkinson's disease more frequent with pramipexole treatment than with placebo were nausea, dyskinesia, hypotension, dizziness, somnolence, insomnia, constipation, hallucination, headache and fatigue. The incidence of somnolence is increased at doses higher than 1.5 mg pramipexole salt per day. A more frequent adverse drug reaction in combination with levodopa was dyskinesia. Hypotension may occur at the beginning of treatment, especially if pramipexole is titrated too fast.
Click on icon to see table/diagram/image
Patient to seek medical attention immediately at the first sight of any adverse drug reaction shall appear.
Carbidopa/Levodopa and Selegiline: Both products did not influence the pharmacokinetics of Pramipexole.
Cimetidine: Cimetidine reduced the renal clearance of pramipexole by approximately 34%, presumably by inhibition of the cationic secretory transport system of the renal tubules. Therefore, medicinal products that are inhibitors of this active renal elimination pathway or are eliminated by this pathway, such as cimetidine, amantadine, and mexiletine, may interact with pramipexole resulting in reduced clearance of either or both medicinal products. Reduction of the pramipexole dose should be considered when these medicinal products are administered concomitantly.
Other drugs eliminated via renal secretion: Population pharmacokinetic analysis suggests that co-administration of drugs that are secreted by the cationic transport system (e.g., ranitidine, diltiazem, triamterene, verapamil, quinidine, and quinine) decreases the oral clearance of pramipexole by about 20%, while those secreted by the anionic transport system (e.g., cephalosporins, penicillins, indomethacin, hydrochlorothiazide, and chlorpropamide) are likely to have little effect on the oral clearance of pramipexole. Other known organic cation transport substrates and/or inhibitors (e.g., cisplatin and procainamide) may also decrease the clearance of pramipexole.
Amantadine: Amantadine may slightly decrease the oral clearance of pramipexole.
Probenecid: Probenecid, a known inhibitor of renal tubular secretion of organic acids via the anionic transporter, did not noticeably influence pramipexole pharmacokinetics.
CYP interactions: Inhibitors of cytochrome P450 enzymes would not be expected to affect pramipexole elimination because pramipexole is not appreciably metabolized by these enzymes in vivo or in vitro. Pramipexole does not inhibit CYP enzymes CYP1A2, CYP2C9, CYP2C19, CYP2E1, and CYP3A4.
Caution is advised when other sedating drugs or alcohol are used with pramipexole because of possible additive effects and the risk of precipitating sudden onset of sleep.
Store at temperatures not exceeding 25°C. Protect from light.
N04BC05 - pramipexole ; Belongs to the class of dopamine agonist. Used in the management of Parkinson's disease.
Ramipex 0.25 tab 250 mcg
30's (P1,140/box)
Ramipex 1 tab 1 mg
30's (P2,550/box)


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image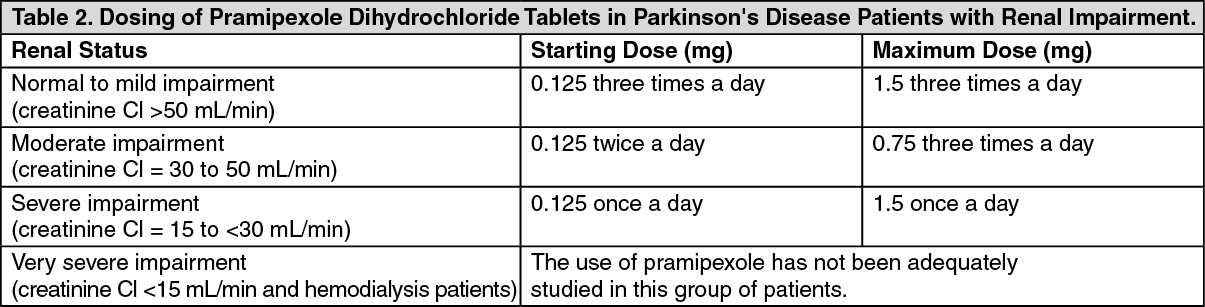 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image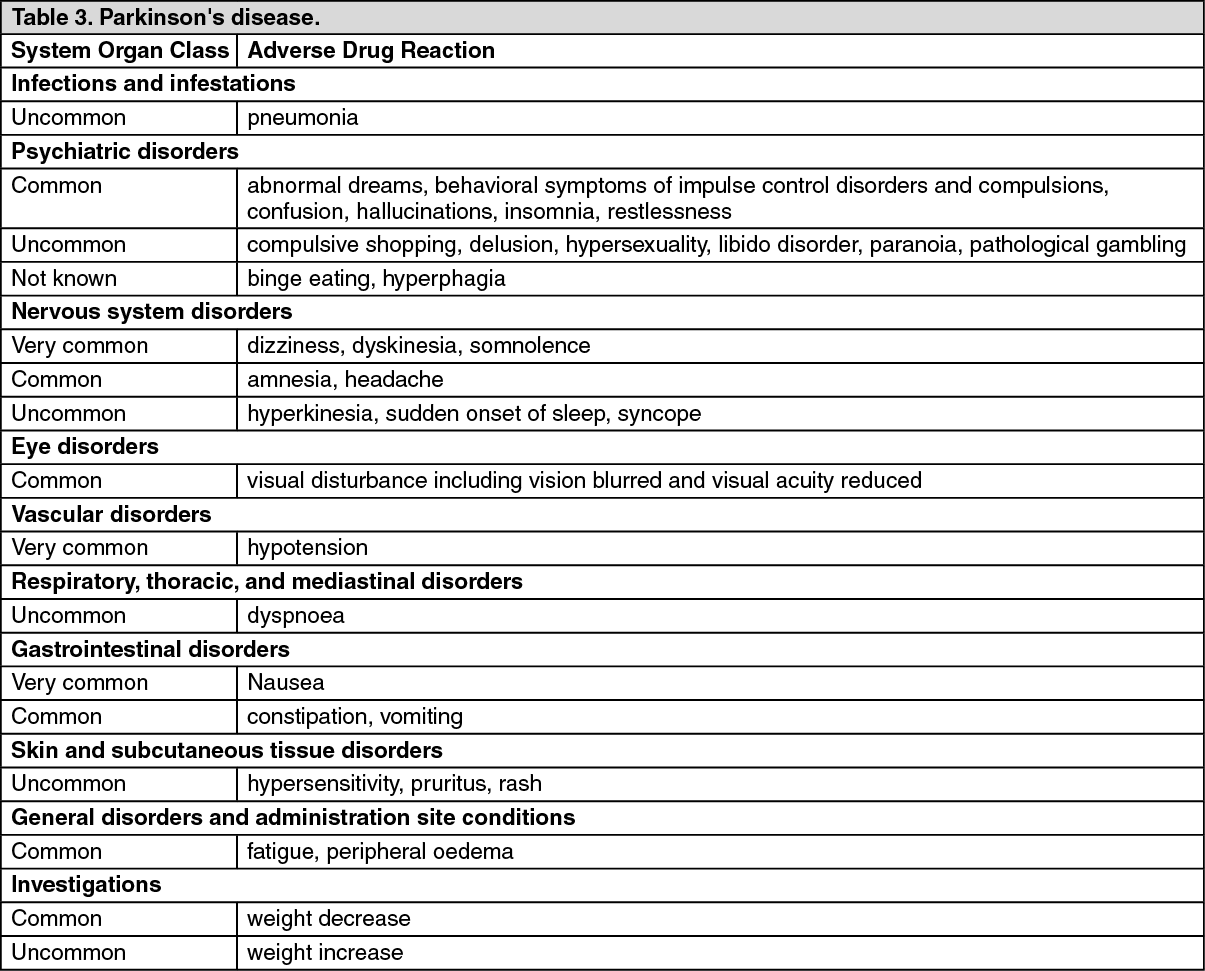 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
